
Knee pain has a way of wearing people down.
Maybe it started gradually. Maybe it followed a workout, a run, or a minor twist that seemed insignificant at the time. You rested. You iced. You modified activity. Maybe you even went to physical therapy — and yet, weeks or months later, your knee still doesn’t feel right.
If your knee has been hurting for months, or if the pain seems to come and go without a clear reason, you’re not alone. This is one of the most common frustrations we hear from patients, especially those who feel like they’ve done everything they were “supposed” to do.
Often, the issue isn’t that something is structurally wrong with your knee. It’s that the deeper contributors haven’t been fully identified or addressed.
When Knee Pain Doesn’t Resolve, It’s Rarely Just About the Knee
The knee sits between two major force-producing regions of the body: the hip above and the ankle and foot below. Its primary role is not to generate power, but to transfer and absorb force efficiently during movement.
When knee pain becomes persistent, it’s often because the knee is compensating for something else that isn’t doing its job well. That compensation may be subtle, and it may have been present long before pain appeared. Over time, however, the knee becomes the place where stress accumulates.
This doesn’t mean your pain isn’t real or that it’s “all coming from somewhere else.” It means the body functions as an integrated system. When one part of that system isn’t contributing effectively, another part often takes on more load — until it starts to complain. Many factors that drive ongoing knee pain originate outside the knee itself, and clinicians and patients often overlook them early on.
Why Rest Often Helps… Until It Doesn’t
Rest can be helpful early on. Reducing activity often calms symptoms and gives irritated tissues a chance to settle. For many people, this brings temporary relief — which can be reassuring at first.
The problem is that rest alone doesn’t build capacity.
When activity drops off for weeks or months, muscles lose strength and coordination, joints experience less load, and movement patterns often become more guarded. Over time, confidence in the knee quietly erodes. When daily activities or exercise resume, the knee must suddenly handle forces it hasn’t been prepared for.
This is why knee pain so often improves, then returns. The symptoms quiet down, but the system itself never fully adapts.
Common Reasons Knee Pain Persists
Persistent knee pain is rarely driven by a single factor. More often, it reflects a combination of movement habits, mobility limitations, and load management issues that build up over time.
The Hip and Ankle May Be Quietly Overloading the Knee
The hip and ankle play a major role in how force moves through the knee.
Limited ankle mobility — particularly reduced ability for the knee to move forward over the foot — can change how the knee bends and absorbs load during walking, squatting, or stair use. This is common after ankle sprains, prolonged sitting, or years of wearing stiff or elevated footwear.
Similarly, inadequate hip control can allow excessive inward collapse or rotation of the thigh. With repeated exposure, the knee absorbs stress beyond what it can efficiently manage on its own. These patterns don’t always cause immediate pain, but over time they increase joint stress and reduce efficiency.
Movement Patterns That Accumulate Stress Over Time
Knee pain rarely stems from one obvious mistake. It develops from repeated exposure to stress that exceeds what the tissues are prepared to tolerate.
Small inefficiencies — such as overstriding while running, shifting weight unevenly, or relying heavily on the knee during bending — may seem insignificant in isolation. But when repeated thousands of times, they add up.
These patterns are rarely intentional and often occur without discomfort at first. Pain typically shows up only after the knee reaches its threshold.
Core and Pelvic Control Influence Knee Load
What happens above the knee also influences how it handles load.
Poor control of the pelvis and trunk can alter lower-body mechanics, changing how force travels through the hip, knee, and ankle. This often shows up as knee pain on one side, knee pain accompanied by hip or low back discomfort, or difficulty controlling single-leg movements.
Without a stable base from the trunk and pelvis, the knee often has to manage forces it can’t efficiently handle on its own.
Why Imaging and Labels Don’t Always Explain Ongoing Knee Pain
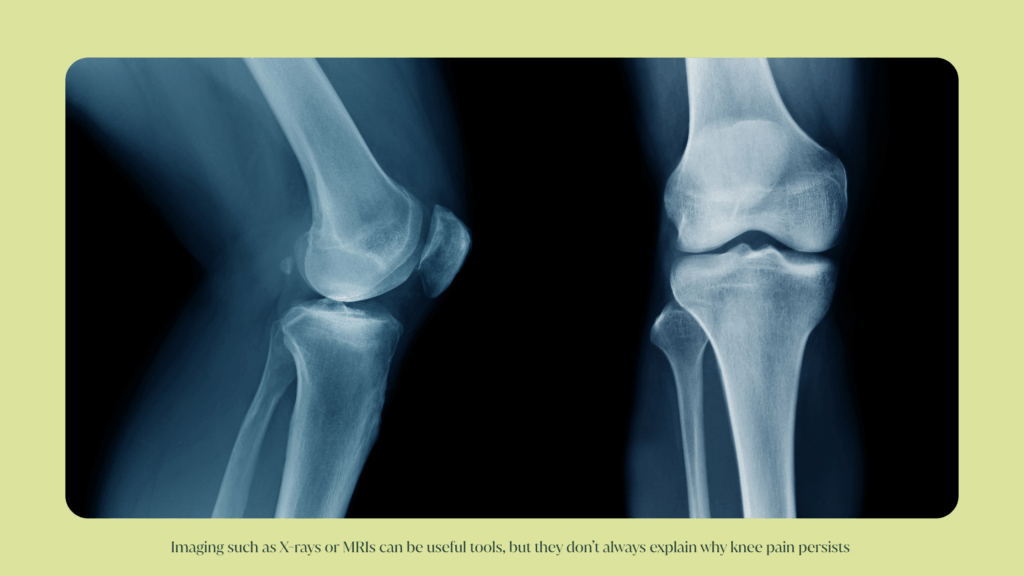
Imaging such as X-rays or MRIs can be useful tools, but they don’t always explain why knee pain persists.
Many findings commonly associated with knee pain — cartilage changes, degenerative labels, structural “abnormalities” — are also present in people who have no pain at all. At the same time, individuals with persistent symptoms may have imaging that looks relatively normal.
Pain reflects more than tissue structure alone. It emerges from how the body applies load, how well tissues tolerate that load, how efficiently you move, and how sensitized the nervous system becomes after repeated stress or injury.
This is why imaging alone rarely provides clear answers when knee pain has been present for months.
Chronic Knee Pain Is Often a Load and Recovery Mismatch
In many cases, the issue isn’t what you’re doing — it’s how much, how often, and how prepared your body is to handle it.
Sudden increases in training volume, intensity, or frequency can overload tissues that haven’t had time to adapt. Daily life stress, poor sleep, and limited recovery can further reduce the body’s ability to tolerate load.
Over time, even well-intentioned movement can become too much for the system. The knee often becomes the place where that overload shows up.
How Physical Therapy Helps When Knee Pain Won’t Go Away
When knee pain has been present for months, physical therapy needs to move beyond symptom relief.
A comprehensive approach looks at how your entire lower body is sharing load, how you move during real-life tasks, and where compensation may be occurring. Treatment focuses on gradually rebuilding strength, coordination, and tolerance while restoring confidence in movement.
The goal isn’t just to eliminate pain. It’s to help the knee — and the system around it — handle daily and recreational demands without repeated flare-ups.
The Takeaway
If your knee pain keeps returning, it doesn’t mean you’ve failed — and it doesn’t mean your knee is broken.
More often, it’s a signal that something in the system hasn’t fully adapted yet. When one area isn’t doing its job well, another often picks up the slack. Over time, that area starts to complain.
Looking beyond the knee — at movement patterns, load, and coordination — is often the missing piece in lasting relief. And that’s where a thoughtful, integrative physical therapy approach can make a meaningful difference.
If you’re still wondering how these ideas apply to your own experience, the questions below address some of the most common concerns we hear from people dealing with ongoing knee pain.
FAQs
Knee pain often develops gradually when the joint repeatedly absorbs more stress than it’s prepared to handle, even without a clear injury. Subtle movement patterns, limited mobility in nearby joints, or changes in activity load can build up over time. Imaging often fails to tell the full story, especially when the body’s ability to manage stress — rather than structural damage — drives pain.
Knee pain that comes and goes is often related to changes in activity level, load, and recovery. Symptoms often settle with rest, then return when the knee has to handle more than it’s currently adapted for. This fluctuation doesn’t necessarily mean new injury — it often reflects a mismatch between capacity and demand.
Rest can reduce symptoms temporarily, and strengthening can help — but knee pain often persists when contributing factors elsewhere in the body aren’t addressed. The hip, ankle, core, and overall movement patterns all influence how much stress the knee absorbs. Without improving how the system works together, progress can plateau even with consistent effort.



